Nuchal translucency (NT) screening is one of the biggest steps forward in prenatal care. It gives expectant parents and clinicians an early look at how a pregnancy is developing. This guide pulls together the science behind NT screening, how it's used in clinic, and where it fits into modern prenatal care, all backed by current evidence.
What is Nuchal Translucency?
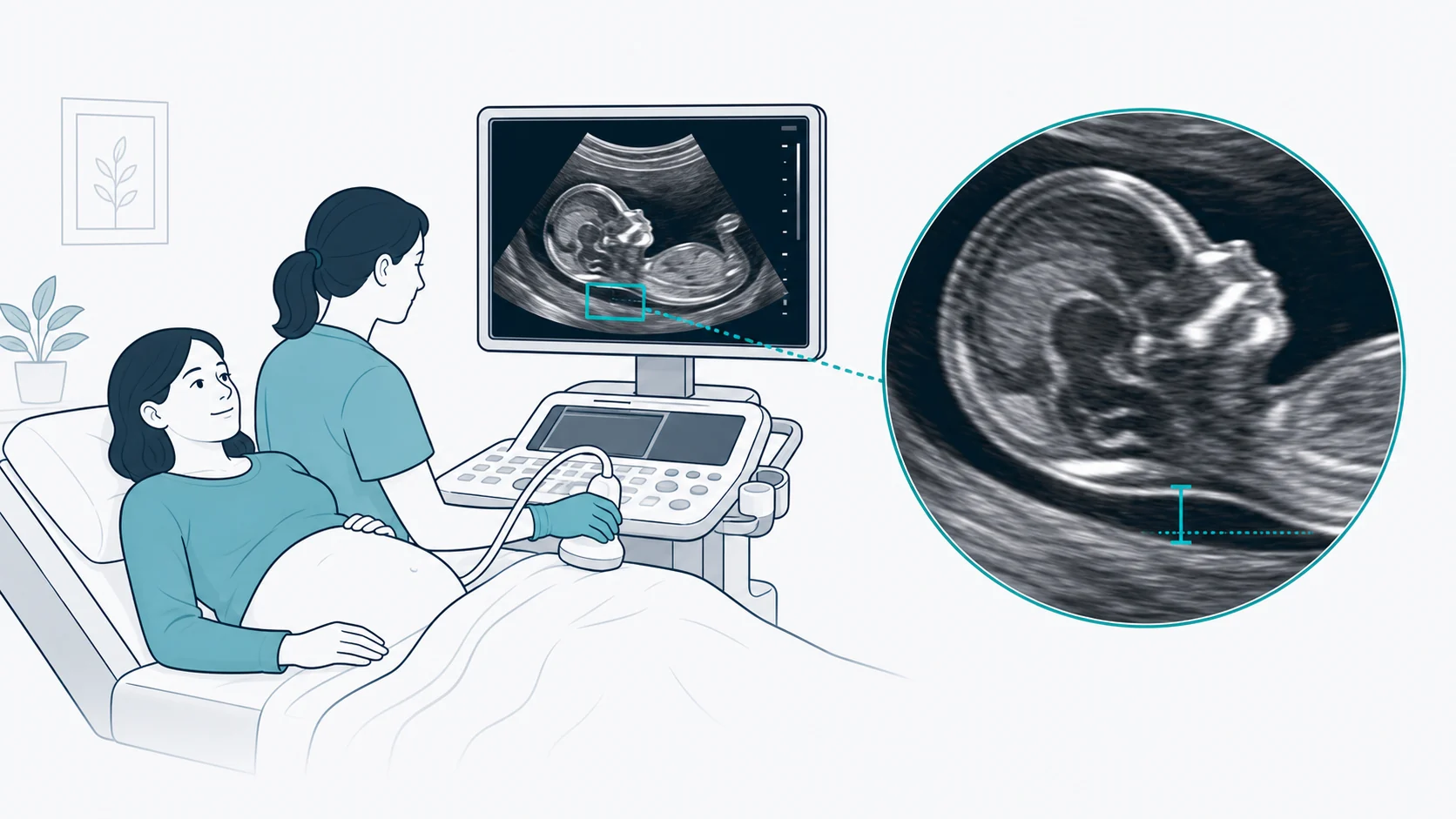
Nuchal translucency (NT) is a small pocket of fluid sitting under the skin at the back of the baby's neck. You can see it on ultrasound in the first trimester. Every fetus has one in early pregnancy. On the scan it shows up as a dark, fluid-filled space between the soft tissue over the cervical spine and the skin above it.
Key Definition
Nuchal Translucency: a sonolucent (anechoic) pocket of fluid sitting under the skin at the back of the fetal neck. We measure it between 11+0 and 13+6 weeks of gestation, when the crown-rump length (CRL) sits between 45-84mm.
Physiological Basis
A few different physiological mechanisms seem to drive fluid buildup in the nuchal region:
- Cardiac Function: Abnormal or delayed cardiac function leading to venous congestion in the head and neck
- Lymphatic Development: Delayed development of the lymphatic system
- Extracellular Matrix: Altered composition of the extracellular matrix in connective tissue
- Fetal Movements: Reduced fetal movements affecting lymphatic drainage
- Connective Tissue: Underlying connective tissue disorders associated with certain syndromes
As the fetal lymphatic system matures and cardiac function picks up, this fluid usually gets reabsorbed. In most cases, NT settles by the end of the first trimester. When the fluid build-up is excessive though, it can point to fetal conditions that need a closer look.
The Critical Timing Window
Optimal NT Measurement Timing
- Gestational Age – 11+0 to 13+6 weeks
- Crown-Rump Length – 45-84mm
- Optimal CRL – 63mm (12+3 weeks)
Why This Timing Matters
The 11+0 to 13+6 week window isn't pulled out of thin air. It comes down to a few clinical and biological reasons:
- Before 11 weeks: Technical difficulties in obtaining accurate measurements due to small fetal size
- After 14 weeks: Normal lymphatic system development causes fluid reabsorption, reducing sensitivity
- 12+3 weeks (CRL ~63mm): Optimal balance between image quality and detection sensitivity
Normal NT Values by Gestational Age
| CRL (mm) | Median NT (mm) | 95th Percentile (mm) | 99th Percentile (mm) |
|---|---|---|---|
| 45 | 1.2 | 2.0 | 2.5 |
| 55 | 1.4 | 2.2 | 2.8 |
| 65 | 1.5 | 2.4 | 3.0 |
| 75 | 1.7 | 2.6 | 3.2 |
| 84 | 1.8 | 2.8 | 3.4 |
Note: if NT measures above the 95th percentile (usually 3.5mm), it needs further investigation no matter what the screening test says. As NT thickness goes up, so does the risk of poor outcomes.
Detection Rates and Accuracy
NT measurement on its own is useful, but pair it with other markers and accuracy jumps a lot. First-trimester screening has steadily improved over the years, and the numbers show it:
| Method | Detection rate (Trisomy 21) | Notes |
|---|---|---|
| NT Alone | 70-75% | A single measurement that gives baseline screening on its own. ~5% False Positive Rate. |
| Combined Screening | 85-90% | NT + PAPP-A + free β-hCG + Maternal Age. ~5% False Positive Rate. |
| Enhanced Screening | 93-96% | Combined + Nasal Bone + Tricuspid Flow + Ductus Venosus. ~2.5% False Positive Rate. |
Additional First-Trimester Markers
Chromosomal Abnormalities and NT Thickness
An increased NT measurement is linked with a range of chromosomal abnormalities, and the risk climbs as NT gets thicker. Knowing these links shapes how you counsel families and plan follow-up care.
Cardiac Risk Assessment
One of the biggest uses for NT measurement is cardiac risk assessment. Congenital heart defects (CHD) sit among the most common structural abnormalities, and an elevated NT is a useful marker that flags babies for a closer cardiac look.
CHD Risk by NT Thickness
Outcome Prediction with Elevated NT
When NT is elevated but chromosomes come back normal, parents need clear answers about what that actually means for their pregnancy. Research now maps out clear links between NT thickness and outcomes.
Normal Outcome Rates (Chromosomally Normal Fetuses)
First-Trimester Combined Screening Protocol
Modern first-trimester screening pulls together several components to lift detection while keeping false positives low. Combined screening is now the gold standard for an initial prenatal assessment.
- NT Measurement: correct technique with a mid-sagittal view and neutral fetal position
- Crown-Rump Length: for accurate gestational age dating
- Nasal Bone Assessment: present, absent, or hypoplastic
- Optional: tricuspid flow and ductus venosus assessment
- PAPP-A (Pregnancy-Associated Plasma Protein-A): typically low in aneuploidies
- Free β-hCG: higher in trisomy 21, lower in trisomies 13 and 18
- Best Timing: blood draw ideally at 10-11 weeks, though it can be done up to 13+6
- Results Expression: reported as Multiples of Median (MoM)
Quality Assurance in NT Measurement
Accurate NT measurement comes down to standardised technique, proper training, and ongoing quality assurance. Certification programs keep practitioners working to a high standard.
Certification Requirements
- Online theoretical training
- Image submission for assessment
- Annual re-certification
- Ongoing audit requirements
- Local accreditation standards
- Regular performance audits
- Statistical outcome monitoring
- Continuous education requirements
Quality Benchmarks
Clinical Management Pathways
After NT screening, what you do next depends on the calculated risk and the NT measurement itself. Clear pathways keep follow-up on track for every risk category.
- Routine prenatal care
- Standard second trimester anatomy scan
- Reassurance counselling
- Offer cell-free DNA (NIPT) testing
- Discuss options including invasive testing
- Consider additional first trimester markers
- Enhanced second trimester scan
- Offer invasive diagnostic testing (CVS/amnio)
- Detailed early anatomy scan
- Fetal echocardiography at 16-18 weeks
- Referral to maternal-fetal medicine
- Genetic counselling
Key Counselling Principles
Special Clinical Scenarios
Multiple Pregnancies
In a multiple pregnancy, you need to assess each fetus on its own and pay close attention to chorionicity. In monochorionic twins, NT discordance can point to twin-to-twin transfusion syndrome (TTTS) or selective intrauterine growth restriction.
- Assess each fetus on its own
- Remember chorionicity changes how you read results
- A higher NT in one twin can flag TTTS risk
- Combined screening is less accurate in multiples
Failed NT Measurement
Sometimes the measurement just isn't possible. An awkward fetal position or maternal habitus can get in the way. When that happens, offer alternatives:
- Repeat the scan within 48-72 hours
- Use second trimester serum screening (Quad test)
- Consider NIPT as another screening option
- Document why the scan failed in the records
Cystic Hygroma vs. Increased NT
Telling nuchal oedema and cystic hygroma apart matters for prognosis. A cystic hygroma, which shows septations, carries a higher risk of aneuploidy and a poorer outcome than a plain increased NT.
- Septated hygroma carries around 50% aneuploidy risk
- Stronger link with Turner syndrome
- Poorer prognosis even with normal chromosomes
- Needs an early, detailed anatomy evaluation
Limitations of NT Screening
- Not diagnostic: you'll need confirmatory testing for a definitive diagnosis
- Narrow window: must be done within a specific gestational age range
- Operator dependent: accuracy depends heavily on practitioner skill and certification
- False positives: roughly 5% of normal pregnancies will still screen positive
- Technical factors: maternal habitus and fetal position can both limit the assessment
- Won't pick up everything: some conditions just aren't linked to an increased NT
Conclusion
Nuchal translucency screening has reshaped first-trimester prenatal care. It gives early, non-invasive insight into fetal risk for chromosomal abnormalities, cardiac defects, and other structural anomalies. Pair it with maternal serum biochemistry and a few extra ultrasound markers and detection rates climb to excellent levels while false positives stay within an acceptable range.
Clinicians doing NT assessments need to keep their certification and quality standards up to get reliable results. Clear talk about the results, their limits, and the follow-up options available means expectant parents can make informed decisions.
Key Takeaways
- NT screening works best between 11+0 and 13+6 weeks (CRL 45-84mm)
- Combined screening (NT plus biochemistry) hits an 85-90% detection rate for trisomy 21
- An elevated NT needs further investigation no matter what the combined screening says
- Most pregnancies with elevated NT and normal chromosomes go on to have good outcomes
- Quality assurance and certified practitioners are the backbone of reliable results
- Clear, balanced counselling helps patients make informed decisions