
When we send an aged care resident to hospital for an X-ray to rule out a fracture, we think we're doing the right thing. But the research tells a different story - one of delirium, functional decline, and mortality rates that should make us question every transfer decision.
The Numbers We Don't Talk About
Hospital transfers for aged care residents - even for seemingly minor investigations like an X-ray to rule out a fracture - carry significant risks that are often underestimated.
The research reveals concerning statistics about delirium incidence, functional decline, prolonged recovery times, and mortality rates that have major implications for clinical decision-making in residential aged care.
Understanding Delirium: More Than Just Confusion
Delirium is not simply "confusion" or "being a bit muddled." It's a critical neurocognitive disorder characterised by an acute and fluctuating disturbance in attention, awareness, perception, and general cognition.
The Hidden Delirium Problem: "Quiet Delirium"
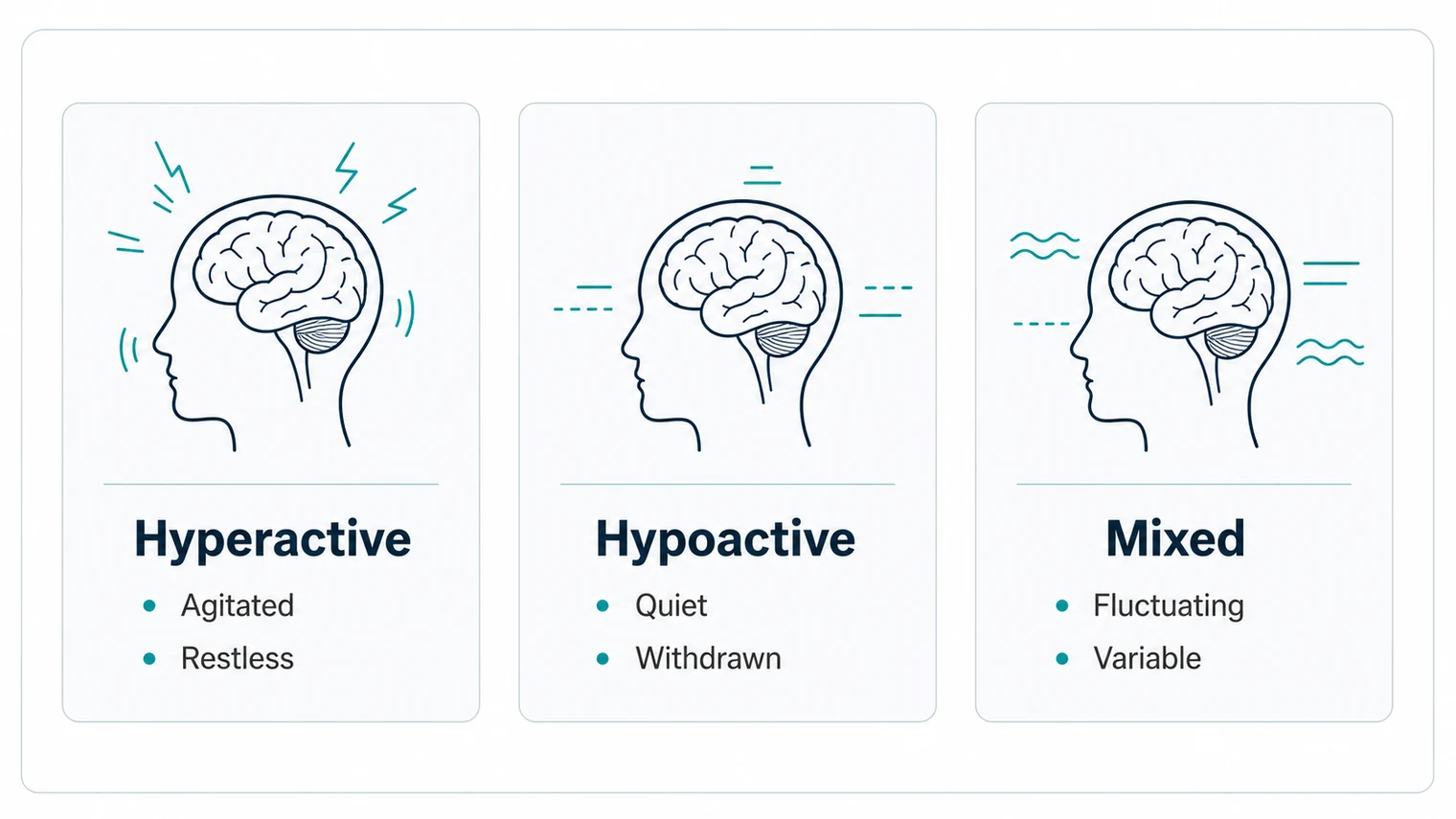
The most common form of delirium in older people is the hypoactive subtype - presenting with reduced motor activity, lethargy, withdrawal, and drowsiness. This "quiet delirium" is frequently missed because patients aren't agitated or disruptive.
50-75% of delirium cases go unrecognised in Emergency Departments.
This means the statistics we present here are likely underestimates. The true harm from undetected delirium is probably far worse than what the research captures.
Understanding Delirium Subtypes
| Subtype | Typical presentation | Recognition |
|---|---|---|
| Hyperactive | Agitation, restlessness; hallucinations; pulling at lines or tubes; wandering, aggression | More easily recognised |
| Hypoactive (most common) | Lethargy, drowsiness; reduced motor activity; withdrawal, flat affect; decreased alertness | Often missed, worse outcomes |
| Mixed | Fluctuates between states; unpredictable presentation; changes throughout the day; often worse at night | Challenging to manage |
Australian Data: The Prevalence Problem
In Australian hospitals, the numbers are stark. The national hospital-acquired delirium rate stands at 51 per 10,000 hospitalisations, making it the most common hospital-acquired complication in Australia.
Nursing home residents face substantially elevated risk compared to community-dwelling elderly. They are three times more likely to present to an emergency department with delirium than those living independently.
Recent research found even higher rates, with 14% incidence among patients newly admitted to medical wards. That suggests earlier estimates may have been conservative.
Risk Factors: Why Your Residents Are Vulnerable

Pre-existing dementia is the single most powerful predictor of both delirium at admission and incident delirium during hospitalisation:
- Delirium at admission: OR 3.18 (95% CI: 1.65 to 6.14)
- Hospital-acquired delirium: OR 4.82 (95% CI: 2.19 to 10.62)
Key insight: The risk of developing delirium during admission is substantially higher than presenting with it. That shows the acute care environment itself is disproportionately damaging to cognitively impaired residents.
The most significant risk factors for delirium among hospitalised aged care residents include:
- Dementia – Residents with dementia have 3-5 times higher odds of developing delirium (OR 3.18-4.82)
- Age Over 65 – Or 45 for Aboriginal and Torres Strait Islander peoples
- Severe Medical Illness – High acuity at presentation increases risk significantly
- Hip Fracture & Orthopaedic Trauma – Particularly high-risk presentations
- Polypharmacy – Anticholinergic medication use increases susceptibility
The Residents Who Never Return
Perhaps the most sobering statistic: a substantial proportion of aged care residents who are transferred to hospital never return to their facility.
In-Hospital Death Rates by Country
The share of transferred aged care residents who die during a hospital admission varies widely between countries. Australia sits in the middle of that range.
| Country | In-hospital death rate |
|---|---|
| Japan | 46.9–77.1% |
| Germany | 28.9–29.5% |
| France | 25.3% |
| Australia | ~22–25% |
| Belgium | 19.7% |
| United States | 17.5% |
| United Kingdom | 10.8–27% |
| Netherlands | 6% |
The median in-hospital death rate for nursing home residents across 29 studies is 22.6%. That's nearly 1 in 4 residents who go to hospital and don't come back.
How quickly deaths occur after hospital admission
| Time after admission | Cumulative share of in-hospital deaths |
|---|---|
| Within 24 hours | 18% |
| Within 3 days | 33% |
| Within 7 days | 59% |
Nearly 6 in 10 nursing home residents who die in hospital die within the first week, suggesting many transfers occur during terminal decline, often without clear advance care planning.
Australian RACF Residents with Dementia
For Australian RACF residents with dementia specifically:
- 6% died during hospital stays
- 29% were transferred to another hospital
- 17% ended up in unplanned new admissions to residential care, meaning they returned to a different facility or higher-level care than their original placement
Recovery: The Long Road Back
One of the most striking findings from the research is how long delirium symptoms persist. This isn't a condition that clears up in a few days.
Delirium Persistence Rates Over Time
Percentage of patients still experiencing delirium symptoms.
| Time after admission | Still experiencing symptoms |
|---|---|
| At Discharge | 36% |
| 1 Month | 33-45% |
| 3 Months | 21-25% |
| 6 Months | 21% |
| 12 Months | 16% |
1 in 3 are still symptomatic at discharge, and 1 in 6 are still affected after 1 year.
Key Insight: Even at 12 months, 16% of patients still haven't fully recovered from delirium. Symptoms can persist for a year or more.
For patients with dementia specifically, the recovery trajectory is even more concerning:
| Full recovery | Patients WITH dementia | Patients WITHOUT dementia |
|---|---|---|
| At 4 weeks | 1% | 4% |
| At 24 weeks | 12% | 27% |
Functional Decline: Getting Worse, Not Better
Beyond delirium, hospital admission triggers broader functional decline that profoundly affects residents' ability to return to baseline:
Hospital-Acquired Functional Decline (HAFD)
Between 34% and 50% of older people experience Hospital-Acquired Functional Decline, losing the ability to perform routine activities of daily living (ADLs) that they could manage before admission.
| Trajectory | Share | Description |
|---|---|---|
| "Decline-no recovery" trajectory | 53% | Pre-admission decline that did not recover during hospitalisation |
| "In-hospital decline" trajectory | 11% | New decline occurring during the hospital stay itself |
Both trajectories were independently associated with higher 6- and 12-month mortality rates.
The Speed of Decline
Functional decline begins remarkably quickly - as early as day 2 of hospitalisation - and for 67% of patients, there is no improvement between day 2 and discharge.
Hospital-Acquired Complications Beyond Delirium
Patients diagnosed with delirium show significantly increased rates of:
- 19% – develop new pressure ulcers (vs 4.3% community-dwelling)
- +8 days – average extended length of hospital stay
- Higher – acquisition of antibiotic-resistant organisms
The Long-Term Consequences
A 2025 meta-analysis of 253 studies (29,814 patients with delirium) quantified the dramatic long-term impacts:
| Outcome | Increased odds | Note |
|---|---|---|
| Incident Dementia | 5.37× | Largest effect observed |
| Institutionalisation | 2.80× | Higher care needs |
| Mortality | 2.55× | Death within follow-up |
| Hospital Readmission | 1.70× | Return to hospital |
The implications are stark: a single episode of hospital-acquired delirium increases the odds of dementia diagnosis by more than five-fold over subsequent years.
The Revolving Door: ED Readmissions
The harm doesn't end with the first transfer. Research shows:
- 37% – re-present to ED within 2 weeks
- 66% – back in ED within 12 months
This high readmission rate reflects unresolved health issues and ongoing decline after the initial "ordeal."
The Avoidable Transfers
The research consistently identifies that many RACF-to-hospital transfers could be avoided with appropriate resources and staffing:
- 40-55% – of ED transfers from Australian RACFs are considered potentially avoidable
- 27,569 – hospital admissions per year from nursing homes are potentially preventable
- $312M – annual cost of these preventable admissions
The X-Ray Problem
A detailed Monash Health study examined RACF transfers specifically for post-fall head injury assessment and found:
- 53% of transfers were classified as "potentially avoidable"
- 76% of the potentially avoidable group underwent CT brain scans
- Only 6% of CT scans showed acute intracranial trauma findings
- None required neurosurgical intervention
Estimated minimum annual cost of potentially avoidable transfers: $1.39 million (transport, ED care, imaging alone)
The Transfer Paradox
In this study, zero patients required neurosurgical intervention, yet every transferred resident was exposed to the cascading risks of delirium, functional decline, and mortality that accompany hospital admission.
A Troubling Finding: Advance Care Directives
The Monash Health study found that the presence of an Advance Care Directive had little bearing on whether imaging was performed, suggesting clinical default practices override documented patient preferences.
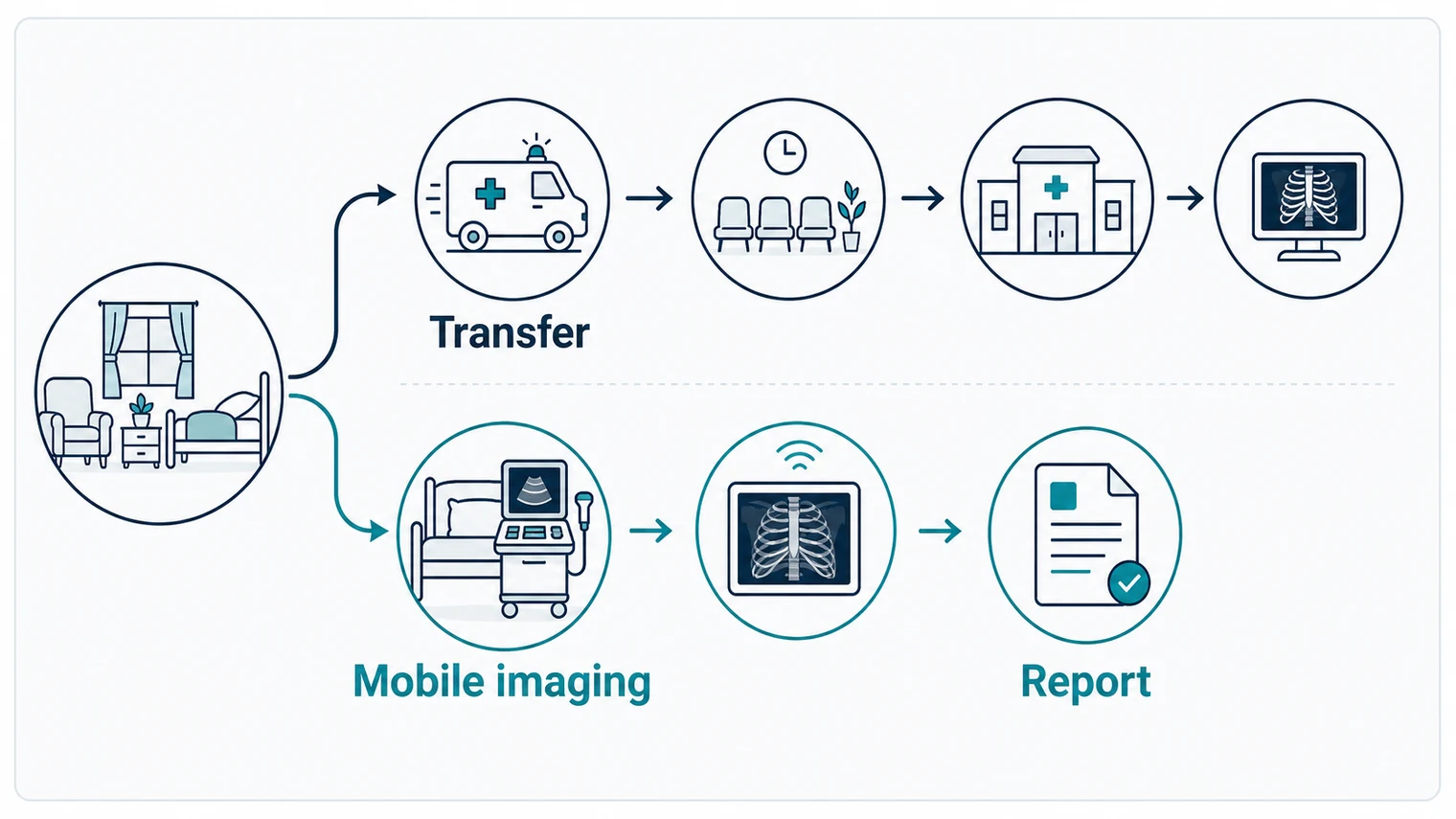
Mobile Imaging: The Alternative That Works

Research on mobile X-ray services (MXS) in nursing homes demonstrates significant potential for reducing transfers. A Victorian study reported an 11.5% reduction in ED presentations requiring plain X-rays following MXS implementation.
Benefits of Mobile Imaging
- Reducing emotional distress for residents
- Avoiding exposure to hospital-acquired complications
- Enabling faster diagnosis and treatment initiation
- Keeping residents in familiar environments with trusted staff
The Cascade of Harm
The evidence suggests that for many aged care residents, particularly those with dementia or significant frailty, hospital transfer initiates a cascade of harm that extends well beyond the initial presenting complaint:
- Acute Phase. 38% develop delirium; 19% develop pressure ulcers
- At Discharge. 36% have persistent delirium symptoms
- Short-Term (3 months). 30% experience functional decline persisting
- Long-Term. 5.4× increased odds of dementia; 2.8× increased institutionalisation risk
Decision-Making Considerations
For investigations like X-rays to rule out fracture, the evidence supports careful consideration of:
- Whether the investigation will change management (given that even positive findings rarely lead to surgical intervention in this population)
- The resident's advance care directive and expressed preferences
- Availability of alternatives such as mobile imaging services
- The cumulative risk of delirium, functional decline, and non-return
For RACF residents with potential intracranial injury post-fall, only 1 in 20 will have intracranial trauma, of whom only 1 in 10 will deteriorate, and neurosurgical intervention is extremely unlikely.
What This Means for Aged Care Professionals
You Can Make a Difference
Every time you consider whether to call an ambulance or arrange a hospital transfer, you're making a decision that could fundamentally alter a resident's trajectory. The research is clear: keeping residents out of hospital whenever safely possible is not just convenient - it's potentially life-saving.
Mobile imaging services offer a genuine alternative that can:
- Provide diagnostic answers without the transfer
- Keep residents in familiar, safe environments
- Reduce the risk of delirium, functional decline, and mortality
- Enable faster clinical decision-making
- Allow family and friends to remain present during care
Protect Your Residents
At Modia Health, we provide mobile X-ray and ultrasound services that come to your facility, helping you avoid unnecessary hospital transfers and the cascade of harm they can cause.
- Same-day urgent service available
- Imaging in the comfort of their room
- CAREPACT integration for eligible residents
- Rapid reporting when it matters most
Related Articles
Delirium Is Preventable
The good news: 30 to 40% of delirium cases are preventable with appropriate interventions.
| Figure | What it represents |
|---|---|
| OR 0.47 | Reduction in delirium incidence with the HELP program |
| 42% | Reduction in falls with multicomponent interventions |
| $16,000+ | Saved per person-year in long-term care costs |
The Hospital Elder Life Program (HELP) and similar non-pharmacological interventions have demonstrated significant efficacy, but the most effective prevention is avoiding unnecessary transfers in the first place.
References & Sources
This article synthesises research from multiple peer-reviewed sources including:
Australian Research
- Australian Commission on Safety and Quality in Health Care - Delirium Clinical Care Standard (2021)
- University of the Sunshine Coast - 2025 delirium prevalence research
- Monash Health study on post-fall transfers from RACFs
- Australian Medical Association reports on preventable aged care admissions
- Victorian mobile X-ray services implementation study
International Meta-Analyses
- Age and Ageing Journal - Systematic reviews on RACF transfers (29 studies)
- 2025 meta-analysis on delirium long-term outcomes (253 studies, 29,814 patients)
- Hospital Elder Life Program (HELP) systematic review
- International comparison of nursing home mortality rates
Key Journals
- Age and Ageing
- BMJ Open
- JAMA Internal Medicine
- Frontiers in Physiology
- The Lancet
This article is intended for informational and educational purposes for aged care professionals. Clinical decisions should always be made in consultation with qualified medical professionals and based on individual patient circumstances.